Association of primary care continuity with outcomes following transition to adult care for adolescents with severe mental illness
Importance — Adolescents with severe mental illness often age out of pediatric care without a clear transfer of care to adult services. The extent to which primary care provides stability during this vulnerable transition period is not known.
Objective — To analyze the association between primary care continuity during the transition from pediatric to adult care and need for acute mental health services in young adulthood.
Design, Setting, and Participants — This population-based cohort study used linked health and demographic administrative data for all adolescents aged 12 to 16 years with severe mental illness ascertained by hospitalization for schizophrenia, eating disorder, or mood disorder between April 1, 2002, and April 1, 2014, in Ontario, Canada. Participants were followed up through March 31, 2017. Data were analyzed from July 2018 to January 2019.
Exposures — Continuous primary care (same physician as baseline [age 12-16 years] always or sometimes), discontinuous primary care (visits to a primary care physician during the transition period who was not the patient’s usual physician), and no primary care during the transition period (age 17-18 years).
Main Outcomes and Measures — Mental health–related hospitalizations and emergency department visits in young adulthood (age 19-26 years) adjusted for sex, rurality, neighborhood income, mental illness type, and health service use before transition.
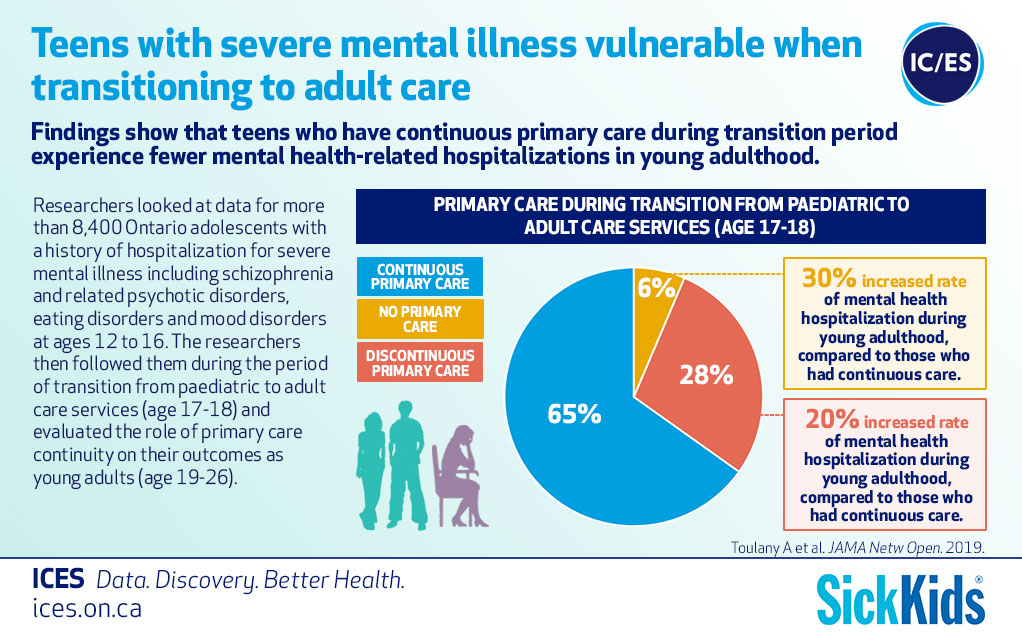
Results — Among 8409 adolescents with severe mental illness (5720 [68.0%] female; mean [SD] age, 14.8 [1.2] years), 5478 (65.1%) had continuous primary care, 2391 (28.4%) had discontinuous primary care, and 540 (6.4%) had no primary care during the transition period. Youths with no primary care during transition were more likely to be male (57.2%), have lower socioeconomic status (31.5%), and have no usual primary care practitioner at baseline (25.6%). Compared with continuous care, patients with discontinuous and no primary care had an increased rate of mental health–related hospitalization in young adulthood (adjusted relative rate, 1.20; 95% CI, 1.10-1.30; and adjusted relative rate, 1.30; 95% CI, 1.08-1.56, respectively).
Conclusions and Relevance — In the context of decreasing outpatient specialist mental health visit rates following transition to adult care, ensuring adequate access to primary care during this vulnerable period may improve mental health outcomes in young adulthood.
Information
Citation
Toulany A, Stukel TA, Kurdyak P, Fu L, Guttmann A. JAMA Netw Open. 2019; 2(8):e198415. Epub 2019 Aug 2.