Predictors of critical care and mortality in bronchiolitis after emergency department discharge
Objectives — To identify the epidemiologic predictors and stratify the risk of critical care (CCU) admission or death in bronchiolitis following ED discharge. This information has not yet been explored.
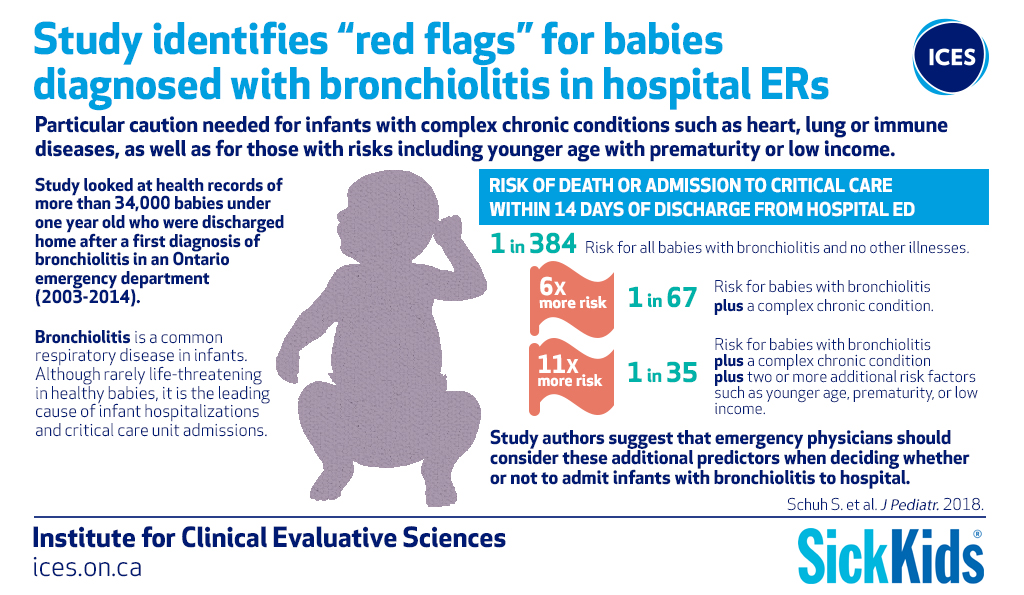
Study Design — A population-based cohort study using Ontario-wide demographic and healthcare Institute for Clinical Evaluative Sciences databases. We assessed all infants with bronchiolitis discharged home from all EDs in Ontario, Canada, 2003-2014. Targeted information included plausible demographic and clinical predictors of CCU admission/death within 14 days of ED discharge. Using multivariable logistic regression analyses we identified independent predictors of this outcome and stratified the outcome risk by the type of multivariable predictor.
Results — Of 34,270 study infants, 102 (0.3%) were admitted to CCU or died after discharge. Predictors of CCU admission/death were: comorbidities (OR5.33; 95% CI 2.82-10.10), younger age [months] (OR1.47; 95%CI 1.33-1.61), low income (OR 1.53; 95% CI 1.01-2.34), younger gestational age [weeks] (OR1.14; 95%CI 1.06-1.22) and emergent presentation (Canadian Triage and Acuity Scale 2) at the index visit (OR1.55, 95% CI 1.03-2.33). The absolute event risk of CCU admission/death in infants with versus without comorbidities were 1.5% versus 0.26%, respectively (p<0.001). The odds of these outcomes in infants with comorbidities plus ≥2 other predictors were one in 35- 25 times higher than in infants without predictors (OR 25.1, 95% CI 11.4-55.3).
Conclusions — Infants with comorbidities plus other predictors discharged from the ED with bronchiolitis are at considerable risk of subsequent CCU admission and death. These risk factors should augment current clinical and social considerations determining patient disposition.
Information
Citation
Schuh S, Kwong J, Holder L, Graves E, Macdonald EM, Finkelstein Y. J Pediatr. 2018; 199:217-22.e1. Epub 2018 May 7.