Do-not-resuscitate and do-not-hospitalize orders in nursing homes: Who gets them and do they make a difference?
Objectives — To describe the rate of do-not-resuscitate (DNR) and do-not-hospitalize (DNH) orders among residents newly admitted into long-term care homes. We also assessed the association between DNR and DNH orders with hospital admissions, deaths in hospital, and survival.
Design — A retrospective cohort study.
Setting and Participants — Admissions in all 640 publicly funded long-term care homes in Ontario, Canada, between January 1, 2010 and March 1, 2012 (n = 49,390).
Measures — We examined if a DNR and/or DNH was recorded on resident's admission assessment. All residents were followed until death, discharge, or end of study to ascertain rates of several outcomes, including death and hospitalization, controlling for resident characteristics.
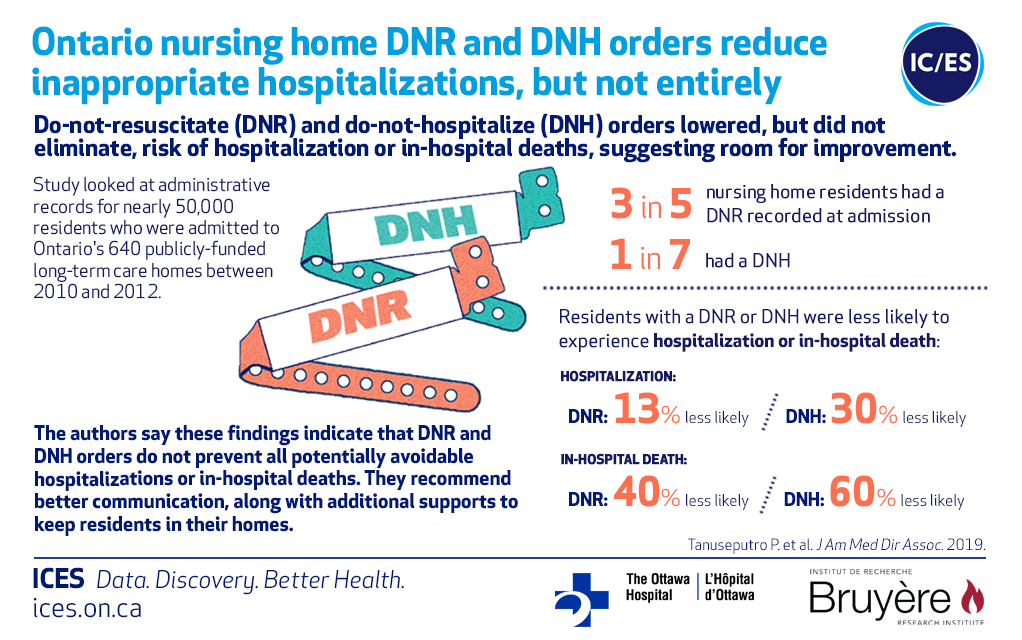
Results — Upon admission, 60.7% of residents were recorded to have a DNR and 14.8% a DNH order. Those who were older, female, widowed, lived in rural facilities, lived in higher income neighborhoods prior to entry, had higher health instability or cognitive impairment, and spoke English or French were more likely to receive a DNR or DNH. Survival time was only slightly shorter for those with a DNR and DNH with a mean of 145 and 133 days, respectively, vs 160 and 153 days for those without a DNR and DNH. After controlling for age, sex, rurality, neighborhood income, marital status, health instability, cognitive performance score, and multimorbidity, DNR and DNH were associated with an odds ratio of 0.57 [95% confidence interval (CI) 0.53-0.62] and 0.41 (95% CI 0.37-0.46) for dying in hospital, respectively. Those with a DNR and DNH, after adjustment, had an incidence rate ratio of 0.87 (95% CI 0.83-0.90) and 0.70 (95% CI 0.67-0.73), respectively, days spent in hospital.
Conclusions and Implications — This study outlines identifiable factors influencing whether residents have a DNR and/or DNH order upon admission. Both orders led to lower rates, but not absolute avoidance, of hospitalizations near and at death.
Information
Citation
Tanuseputro P, Hsu A, Chalifoux M, Talarico R, Kobewka D, Scott M, Kyeremanteng K, Perri G. J Am Med Dir Assoc. 2019; 20(9):1169-74 e1. Epub 2019 Apr 8.