Fragmented care in assisted living linked to lower family doctor attachment
Older adults residing within retirement homes in Ontario are less likely to have a regular family physician for ongoing care than other older adults.
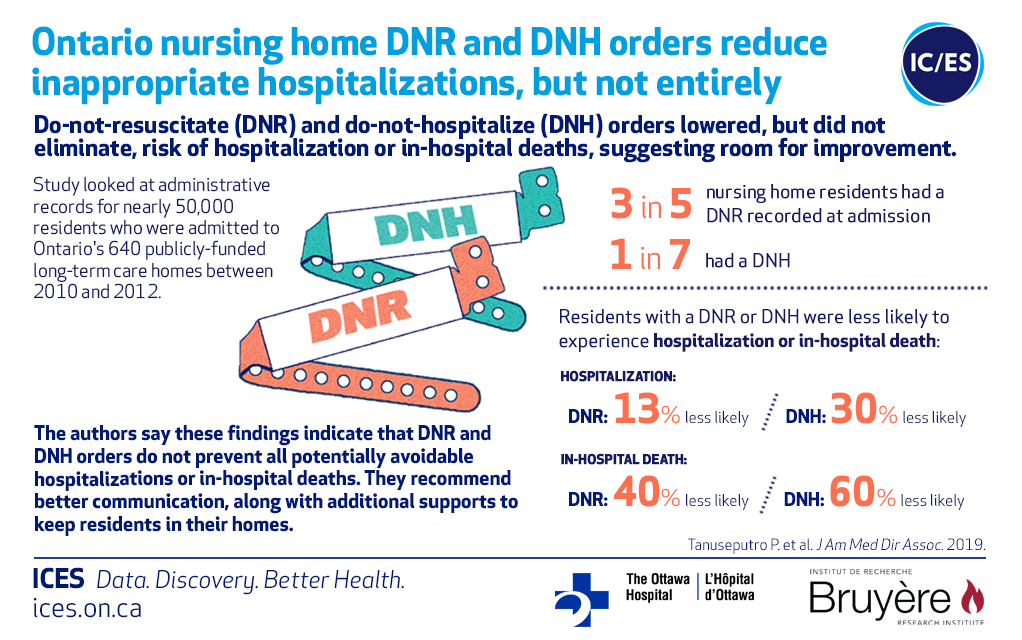
Do-not-resuscitate (DNR) and do-not-hospitalize (DNH) orders in long-term care homes (nursing homes) across Ontario led to reductions in rates of hospitalizations and hospital deaths, but did not eliminate these potentially inappropriate transfers, according to a new study by researchers at ICES, a non-profit research institute that uses population-based health information to produce knowledge on a broad range of healthcare issues.
The study, published today in the Journal of the American Medical Directors Association, is the first to examine which, and how many residents have DNR and DNH orders upon admission to nursing homes across Ontario.
“More and more residents who are admitted to long-term care facilities have a diagnosis of dementia and multiple other diseases, and many are near the end of life. Because of this, nursing homes – which provide care through nurses, doctors, personal support workers, and other providers – are an important setting for palliative and end-of-life care. Decision making about transfers to hospital should be grounded in a shared understanding of prognosis and the resident’s goals and wishes,” says Dr. Peter Tanuseputro, the lead author of the study, adjunct scientist at ICES, researcher at the Bruyère Research Institute, staff physician and associate scientist at The Ottawa Hospital and assistant professor in the division of palliative care at the University of Ottawa.
The researchers looked at all admissions, in all 640 publicly-funded long-term care homes in Ontario, between January 1, 2010 and March 1, 2012. Nearly 50,000 seniors were admitted during the study period and followed until death, discharge, or the end of study.
The study showed that approximately three in five (60.7 per cent) residents had a DNR on admission, and only one in seven (14.7 per cent) had a DNH. The researchers found that those who have a DNH had a 60 per cent reduction in hospital deaths, and a 30 per cent reduction in hospital stays. Many residents with such orders, however, are still being transferred and dying in hospital.
“While some of these transfers might be completely appropriate, some may be considered overly aggressive and burdensome. What we found was that DNR and DNH orders are not enough to prevent potentially avoidable hospital visits. Instead, the orders need to be explored with explanations about why these orders are in place, and we need to provide additional supports to keep residents in their home,” says Tanuseputro.
In addition, women, those in living in rural settings, those living in richer neighborhoods prior to entry and those who spoke English or French had higher rates of DNR and DNH. Conversely, residents who did not speak one of the two official languages of Canada had much lower rates of DNR and DNH. For example, DNH rates were 4.6 per cent for East Asians and 6.3 per cent for South, Central and Western Asians compared with 15.7 per cent for English speakers.
The researchers stress that DNR and DNH orders did not lead to an absolute avoidance of hospitalizations near and at death, despite nursing homes being equipped to handle the dying process for the vast majority of residents.
Author block: Peter Tanuseputro, Amy Hsu, Mathieu Chalifoux, Robert Talarico, Daniel Kobewka, Mary Scott, Kwadwo Kyeremanteng, and Giulia Perri.
The study “Do-not-resuscitate and do-not-hospitalize orders in nursing homes: who gets them and do they make a difference?” was published online on April 8, 2019 in the Journal of the American Medical Directors Association.
ICES is an independent, non-profit research institute that uses population-based health information to produce knowledge on a broad range of healthcare issues. Our unbiased evidence provides measures of health system performance, a clearer understanding of the shifting healthcare needs of Ontarians, and a stimulus for discussion of practical solutions to optimize scarce resources. ICES knowledge is highly regarded in Canada and abroad, and is widely used by government, hospitals, planners, and practitioners to make decisions about care delivery and to develop policy. In October 2018, the institute formerly known as the Institute for Clinical Evaluative Sciences formally adopted the initialism ICES as its official name. For the latest ICES news, follow us on Twitter: @ICESOntario
Deborah Creatura
Media Advisor, ICES
[email protected]
(o) 416-480-4780 or (c) 647-406-5996
